.png)
Meet The Best Gastroenterologist in West Delhi - Dr. Sawan Bopanna
Giving Each Patient Compassion They Need.
Designation
Dr Sawan Bopanna
MD(Internal medicine,VMMC and Safadrajang Hospital), DM(Gastroenterology,AIIMS,New Delhi)
Consultant Gastroenterology,
Hepatology and Endoscopy
Senior Consultant
Action Gastrosciences and Liver Institute
Action Balaji Medical Institute
INTRODUCTION
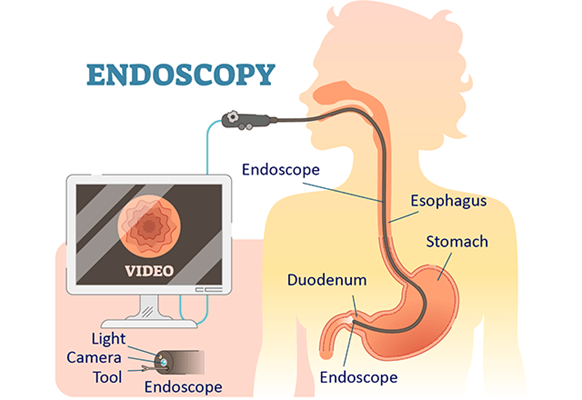
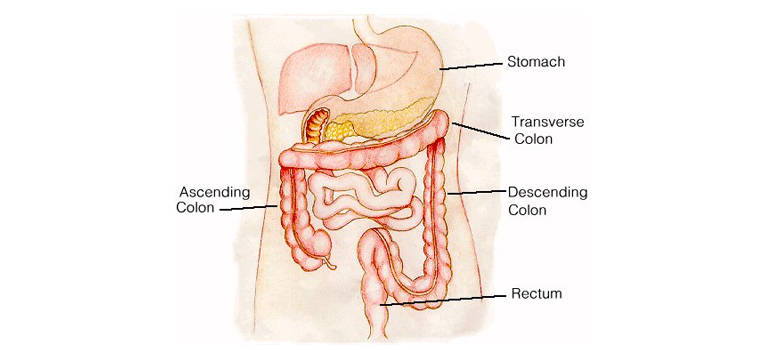
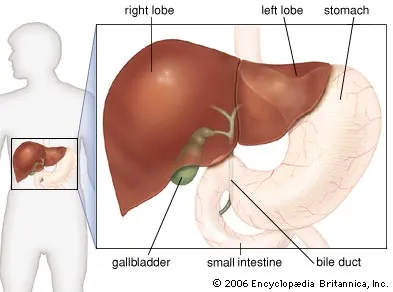
Dr Sawan Bopanna is a practicing consultant in Gastroenterology, Hepatology and Endoscopy in New Delhi. In a career spanning more than 13 years he has established himself as a doctor par excellence. "He previously served as a Senior Consultant at the Max Centre for Gastroenterology, Hepatology, and Endoscopy located at Max Superspeciality Hospital, Saket. Currently, he holds the position of Senior Consultant at the Department of Action Gastrosciences and Liver Institute within Action Balaji Medical Institute, Delhi." Being the best gastroenterologist in West Delhi, he has wide range of experience in treating complex diseases of the liver and gastrointestinal tract. His practice also includes performing advanced endoscopic procedures to cure gastrointestinal ailments. His strong forte is in performing endoscopic procedures like ERCP, endosonography and third space procedures.
Working in a centre with a wide range of evidence based treatment options for all liver and gastrointestinal diseases, patients may choose the most appropriate and cost effective treatment options all gastrointestinal problems. he known as a gastrology doctor in delhi, who ensure Ethical and reliable care with full disclosure to patients regarding advantages and disadvantages in his core priority
He received his training in prestigious medical institutions like Kasturba Medical College, Mangalore, Manipal Academy of Higher Education(MAHE), MD in Internal Medicine from VMMC and Safdarjung Hospital and DM in Gastroenterology from the All India Institute of Medical Sciences(AIIMS, New Delhi).
A keen academician with an active interest in research, he has many publications to his credit. He has contributed to various journals of national and international repute and published in these journals. He had been invited to faculty at various national conferences. He has presented various posters and papers at different conferences. He had made contributions to chapters and e-resources. He is one of the best gastroenterologists in west delhi and the best gastroenterologist in delhi NCR, provide one roof solution so to learn more about your condition book your consultation now
Booking Here Now
When should you consult to the best gastroenterologist doctor in west delhi ?
Reach out when you’re suffering from either of these symptoms








Services available at Gastro Liv Clinic

TESTIMONIALS
Mudita Malik
The Doctor listened to my problem with a lot of patience, gave good attention. He gave a very clear diagnosis and clarified all my doubts. He is very welcoming. I highly recommend.
Noor Noor
Nice ambience ,good faculty and good result especially the doctor is very friendly and open hearted and with such great assisstance from their side my father was able to recover soon and now he's much better . Would really like to recommend all and you will definitely get better services guaranteed
SHIV KUMAR
Met doctor for my mothers treatment…she was taking pain killers for months for abdominal pain ..he prescribed a endoscopy and diagnosed my mother with peptic ulcer disease after endoscopy..she is fine now after treatment…definitely recommend
Our Photo Gallery











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}